

Ulcerative Colitis
“Patient information sheet”
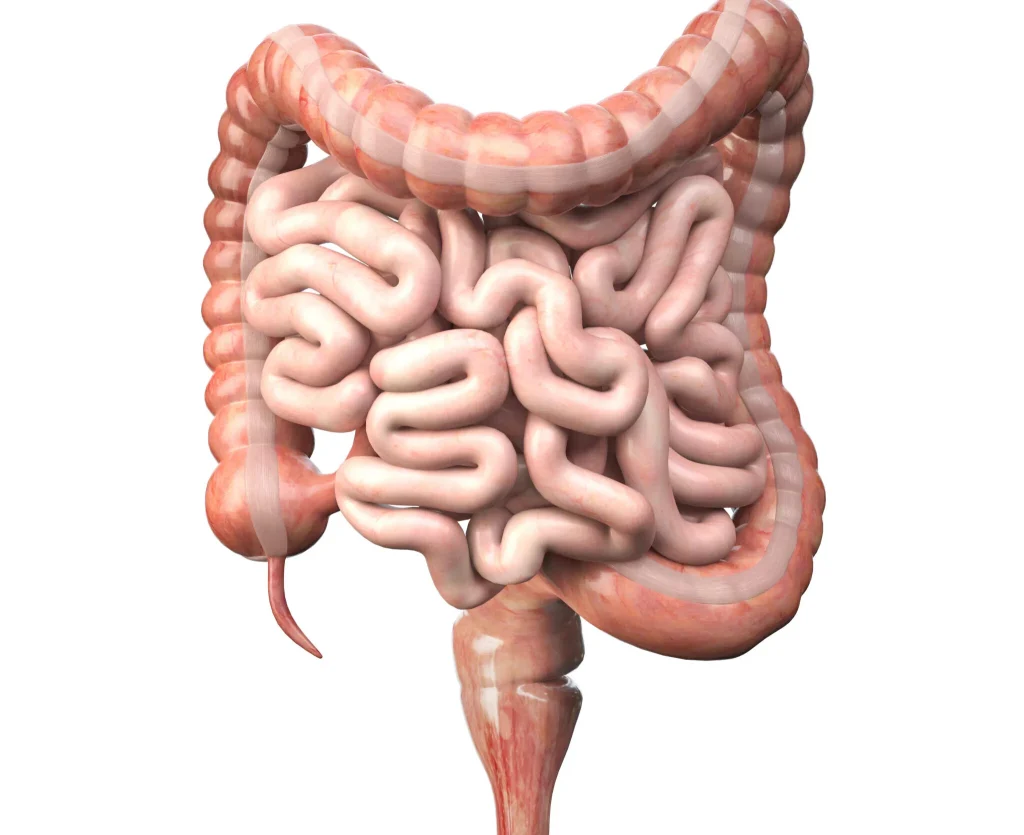
Function of colon
Colon – Also known as large bowel or large intestine is a long, coiled, tube like organ that connects the small instestine to anus. The principal function of the colon is to absorb excess water and salts from the waste material ( left after food has been digested in small intestine), stores solid waste, converting it to stool, and excretes it through the anus.
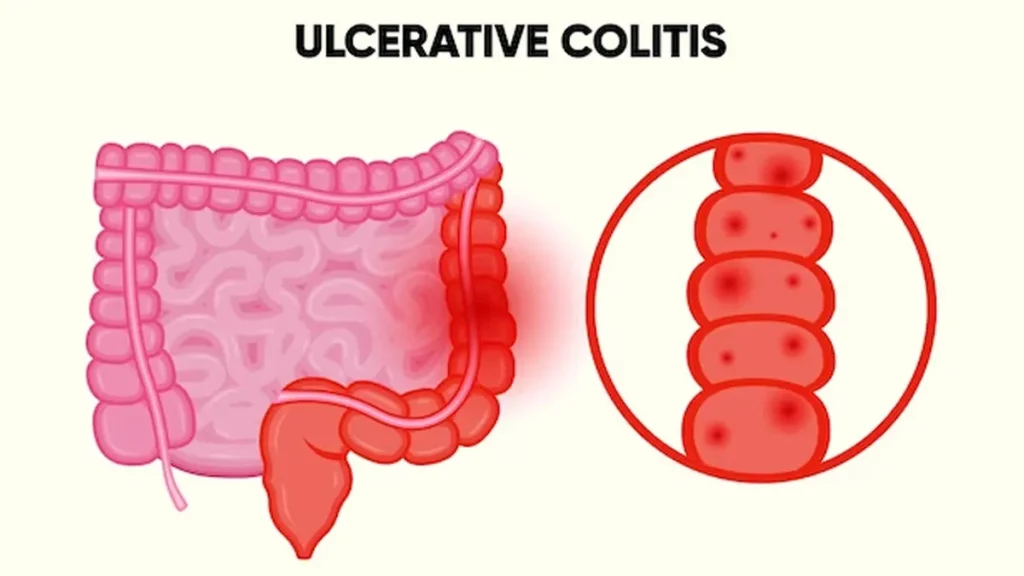
What is Ulcerative Colitis?
Ulcerative colitis (UC) is one of the two main forms of inflammatory bowel disease, also called ‘IBD’. The other main form of IBD is known as crohn’s disease. UC is a chronic inflammatory condition that causes inflammation and ulceration of the inner lining of the rectum and colon (the large bowel). In UC, tiny ulcers develop on the surface of the lining and these may bleed or produce pus. The inflammation usually begins in the rectum and lower colon, but it may affect the entire colon in a continuous manner.
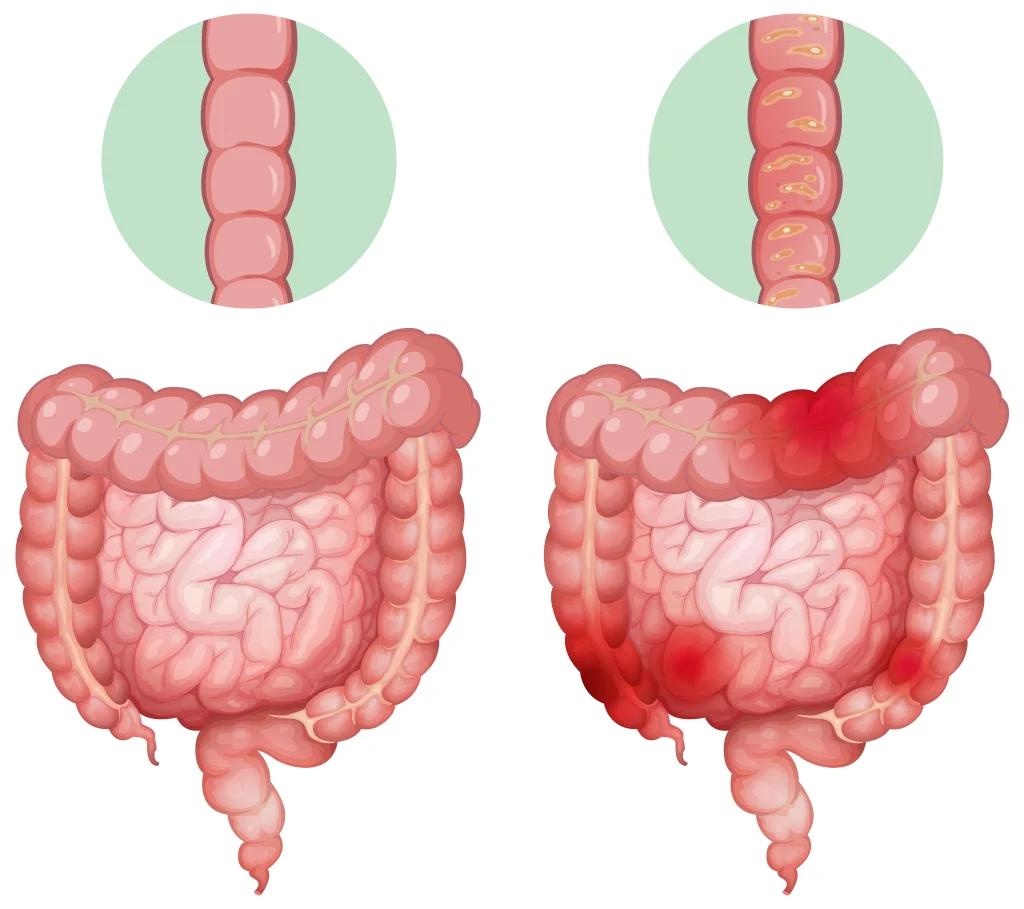
How is ulcerative colitis different from Crohn’s disease?
Crohn’s disease may affect any part of the gastrointestinal (GI) tract, but ulcerative colitis is limited to the colon and rectum. Crohn’s disease can also affect the entire thickness of the bowel wall, while ulcerative colitis only involves the innermost lining of the colon (mucosa /submucosa). Finally, in Crohn’s disease, the inflammation of the intestine can “skip”—leaving normal areas in between patches of diseased intestine. In ulcerative colitis, this does not occur. In only 10 percent of cases are there overlapping features of both ulcerative colitis and Crohn’s disease, a condition called indeterminate colitis.
What causes ulcerative colitis?
“No one knows the exact cause(s) of the disease”
Nothing that you did made you get ulcerative colitis. You didn’t catch it from anyone. It wasn’t something that you ate or drank that brought the symptoms on. So, above all, don’t blame yourself. It is supposed to caused by a combination of factors, including: 1. Genes you are born with, 2. an abnormal reaction of the digestive system to bacteria in the intestine, 3. an unknown ‘trigger’ or set of triggers that could include viruses, other bacteria, diet, stress, or something else in the environment.
What are the symptoms of ulcerative colitis?
Ulcerative colitis is a very individual condition – some people can remain well for a long time, even for many years, while others have frequent flare-ups. They may also change over time, with periods of good health when you have few or no symptoms (remission), alternating with times when your symptoms are more active (relapses or ‘flare-ups’). Most common symptoms during a flare-up are:
- Diarrhoea – often with blood, mucus and pus.
- Cramping pain abdomen – severe, before passing stool.
- Tiredness and fatigue.
- Feeling generally unwell /feverish.
- Loss of appetite and loss of weight.
- Anaemia (if losing a lot of blood in stool)
How severe is my Ulcerative Colitis?

Can Ulcerative Colitis affect other parts of the body?
A variety of symptoms known as extra-intestinal manifestations occur due to involvement of other parts of the body in UC. Signs and symptoms are:
- Eyes ( Episcleritis – redness, pain, and/or changes in vision)
- Mouth (sores)
- Joints ( Acute Arthropathy – – swelling and pain, ankylosing spondylitis ,Sacro-ileitis etc)
- Skin (tender bumps, painful ulcerations, and other sores/rashes, leg -erythema nodosum)
- Liver (primary sclerosing cholangitis and cirrhosis)—a rare development
- In some these signs & symptoms actually may be the first signs of ulcerative colitis, appearing even years before the bowel symptoms. In others, they may occur right before a flare-up.
What are the main types of ulcerative colitis?
Proctitis / proctosigmoiditis
In proctitis, only the rectum is inflamed. The main symptom is passing fresh blood, diarrhoea ( rarely may have normal stool or constipation), urgent need to rush to the toilet. tenesmus. In proctosigmoiditis , the sigmoid colon also is inflamed –symptoms are similar to those of proctitis (but less likely to have constipation).
Left-sided or distal colitis
In this type inflammation starts at the rectum and continues up the left side of the colon (distal or descending colon). Symptoms include diarrhoea with blood and mucus, pain on the left side of abdomen, urgency and tenesmus.
Extensive or Pan Colitis
Extensive colitis extends along most of the colon (upto or beyond transverse colon). It cause very frequent diarrhoea with blood, mucus, and sometimes pus. You may also have severe abdominal cramps and pain, tenesmus, and weight loss. Very rarely, when the inflammation is severe, digestive gases may get trapped in the colon, making it swell up. This is known as toxic megacolon (present as high fever, pain and tenderness in the abdomen) and need urgent surgery.
Can ulcerative colitis lead to bowel cancer?
- Ulcerative colitis is not a form of cancer.
- Patients having extensive or total colitis (pancolitis) for many years (about 8-10 years after the start of the IBD symptoms) have a greater risk than normal of developing cancer in the colon or rectum.
- This increased risk is not as great for people with left sided colitis, and people with proctitis have no increased risk.
- Having Primary Sclerosing Cholangitis (PSC) may also increase risk of cancer.
- A surveillance colonoscopy done in proper time (based on current guidelines and recommendations) will help in early diagnosis of cancer.
- However the overall number of people who develop cancer is very small
- Such cancers can often be more successfully treated if detected early.
How is ulcerative colitis diagnosed?
- Symptoms : If you develop diarrhoea with bleeding and abdominal pain, your doctor may suspect you have ulcerative colitis.
- You will probably be asked to have blood tests like CBC (complete blood count),ESR, CRP (quantitative), Serum Protein/ Albumin to give a measure of the degree of inflammation , anemia and your nutrition level.
- A colonoscopy or sigmoidoscopy – These tests often used to diagnose or monitor progression of colitis. In these tests a sigmoidoscope (a short endoscope) or a colonoscope (a longer and more flexible endoscope) is inserted through the anus (back passage) to examine the innerlayer or mucosa of rectum and colon. These tests should not be painful but may be sometimes uncomfortable, so you may be given a sedative (medication that has a calming effect) to help you relax. Biopsies (small samples of tissue) are often taken to be examined under a microscope to confirm the diagnosis.
- Ultrasound , MRI and CT Scans of abdomen and Pelvis : These tests are used in complicated severe cases to look at the location and extent of inflammation.
What drugs are used to treat ulcerative colitis?
- Drug treatment usually aims to reduce symptoms and control flare-ups, and then to prevent a relapse once the disease is under control.
- This can mean you need to take your medication on an ongoing basis, sometimes for many years.
- Two main types of drugs commonly used in ulcerative colitis are
- (A)Anti-inflammatory drugs – help to reduce inflammation :
- 5-ASAs or aminosalicylates such as mesalazine , sulphasalazine etc. • Corticosteroids, often just called steroids, such as prednisolone, hydrocortisone, budesonide (Entocort) etc,• Immunosuppressants such as azathioprine, Methotrexate, tacrolimus and ciclosporin etc, • Biological or ‘Anti-TNF’ drugs such as infliximab (Remicade) and adalimumab (Humira).
- (B) Symptomatic Drug – help to control and reduce common symptoms:
- Anti-diarrhoeals such as codeine phosphate, diphenoxylate (Lomotil) and Loperamide, • Laxatives such as Movicol and Lactulose ,• Bulking agents,• Analgesics (pain killers) such as paracetamol etc.
- It is best to check with your doctor or IBD team before you take any over-the-counter medicines
What are the most likely operations for ulcerative colitis?
- Ulcerative colitis can often be managed by medication (drug treatment), but surgery may become necessary if the inflammation is very severe, quality of life has been affected by repeated flare-ups .
- People with very severe ulcerative colitis which does not respond to intensive medical treatment will need urgent surgery (within a few days) or emergency surgery (within a few hours).
- About 10-20% of UC patients may eventually need surgery, depending on severity of disease & part affected.
- Surgery may also be recommended if dysplasia (pre-cancerous changes) or cancer is found in your colon during a colonoscopy.
- Most commonly performed surgeries are procto-colectomy with a permanent ileostomy, Restorative proctocolectomy with an ileoanal pouch, Subtotal colectomy with ileorectal anastomosis.
- Recent years there have been great advances and improvements in the design of stoma products, and they are now much more discreet and comfortable. Specialist nurses are usually available to help support you if you have an ileostomy or colostomy.
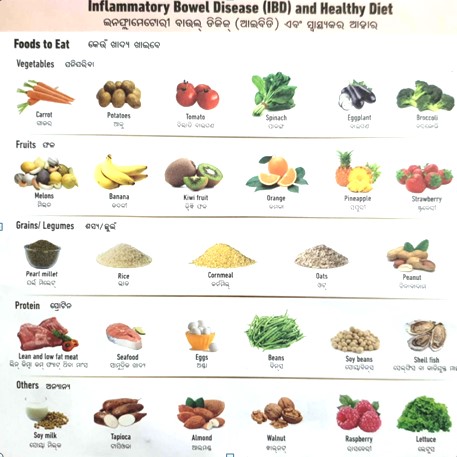
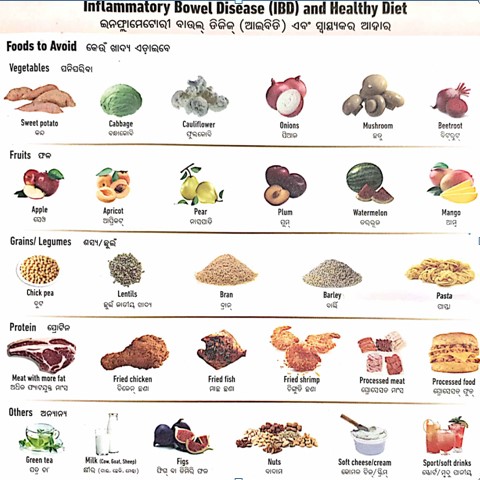
DIET FOR INFLAMMATORY BOWEL DISEASE /colitis
- General information: Most important thing is to eat a nutritious and balanced diet to maintain your weight and strength, and to drink sufficient fluids to stop you getting dehydrated.
- There is no one single diet or eating plan that will relieve the symptoms for every person with with inflammatory bowel disease , but this general information may be helpful.
- Diet during a flare
- During a flare most people find a diet low in fibre and residue helps to relieve symptoms such as cramping and wind. It can also reduce the number of times you pass bowel motions. A low residue diet aims to rest your bowel and allow it to heal.
- A low residue diet involves avoiding roughage (insoluble fibre) that your body struggles to break down. Roughage is found in skins, pips, seeds, whole grain cereals, nuts and raw fruit and vegetables.
- Other food or drinks that can increase bowel motions are spices, greasy food, alcohol, caffeine and fizzy drinks. Often, these dietary changes are temporary and once a flare has resolved efforts should be made to reintroduce fibre gradually.
- Diet during remission (no symptoms)
- If your IBD symptoms are under control (remission), you should be able to eat a well balanced diet. A balanced diet consists of:
- protein sources (meat, fish, poultry or tofu)
- fruit and vegetables
- starchy carbohydrates (bread, rice, pasta or potatoes)
- dairy products (milk, cheese and yoghurt).
- When you are feeling well and are able to eat it is advisable to maintain a healthy weight and keep yourself as well nourished as possible in case your symptoms return.
- There are certain foods that are harder to digest than others. These include skins of fruit, whole grain, brown and wild rice, seeds, pulses (such as peas and beans), nuts, raw fruits and raw vegetables.
What about pregnancy and ulcerative colitis?
- The majority of women with ulcerative colitis can expect a normal pregnancy and a healthy baby. Most women having a baby does not make it worse with IBD.
- If you have ulcerative colitis your chances of conceiving are not usually affected by the disease. But, if you have pouch surgery your fertility could be affected. This appears to be much less likely with a colectomy + ileostomy.
- If you are well when your pregnancy begins you are more likely to have an uncomplicated pregnancy. Also, if you can remain in remission throughout your pregnancy then your chances of a normal pregnancy and a healthy baby are similar to those without IBD.
- Very severe ulcerative colitis can put your baby at greater risk.
- With a few exceptions, most IBD treatment can be continued while you are pregnant. It is generally considered safe to continue taking steroids, most 5-ASAs, and azathioprine, although you should not take methotrexate or mycophenolate mofetil because of an increased risk of birth defects.
Will medicines do harm to the baby if patient is breast feeding?
Breastfeeding is important for the development of a healthy immune system, and is generally recommended.
There is no evidence that many of the drugs used to treat with inflammatory bowel disease are harmful to a breastfed baby, The 5-ASA drugs such as Mesalazine and Sulphasalazine are considered by doctors to be safe while breastfeeding.
Steriods : are generally considered safe, but if you are taking large doses of steroids (over 40mg a day) breastfeeding is not recommended. You can reduce the effects of steroids by waiting for 4 hours after taking a dose before starting to breastfeed.
Azathioprine or Mercaptopurine: Some doctors would not advise breastfeeding, but very little of the active drug is secreted into breast milk. Thus the benefits of may outweigh any small potential risk.
Infliximab : Recent studies suggested does not pass into breast milk and safe to be used.

